CHAPTER 00 // CJC-1295 DAC SOURCING REALITIES
CJC-1295: a long-acting GHRH analog, hand-typed.
Photocopied summaries of the peer-reviewed CJC-1295 record — the pharmacology, the one Phase 1 trial that got published, the one Phase 2 trial that didn't, and the regulatory paper trail that closed the compounding door in 2024.
The short version — what this zine is about
CJC-1295 is a synthetic analog of growth hormone-releasing hormone (GHRH) — a signal the hypothalamus sends to tell the pituitary to release growth hormone. The compound has never been approved for human use anywhere. What it has is one published Phase 1 pharmacology study from 2006, one terminated Phase 2 trial, and a 2024 FDA Pharmacy Compounding Advisory Committee decision that closed the routine compounding door.
The long-acting DAC form bonds covalently to serum albumin in the blood, giving it a half-life of roughly six to eight days — about a thousand times longer than native GHRH [2][3]. The short-acting no-DAC form, marketed as Modified GRF 1-29, lacks that bond and lasts about thirty minutes [6]. They are not the same compound. Most of the popular writing about CJC-1295 mixes them up.
This site does not sell anything and does not give medical advice. It summarizes what the peer-reviewed record and research communities actually report — benefits, side effects, safety cautions, and regulatory paper trail together. See what people report for the community layer.
What this zine is
If you landed here by typing the word get after cjc1295 into a search bar, you already know the editorial problem. CJC-1295 occupies a regulatory grey zone, and most of the writing about it online was assembled by people who wanted to sell something. This site does not sell anything. It is a photocopied reading-room digest of the peer-reviewed record — twenty findings pulled directly from PubMed, ClinicalTrials.gov, and FDA briefing documents, with every quantitative claim cited.
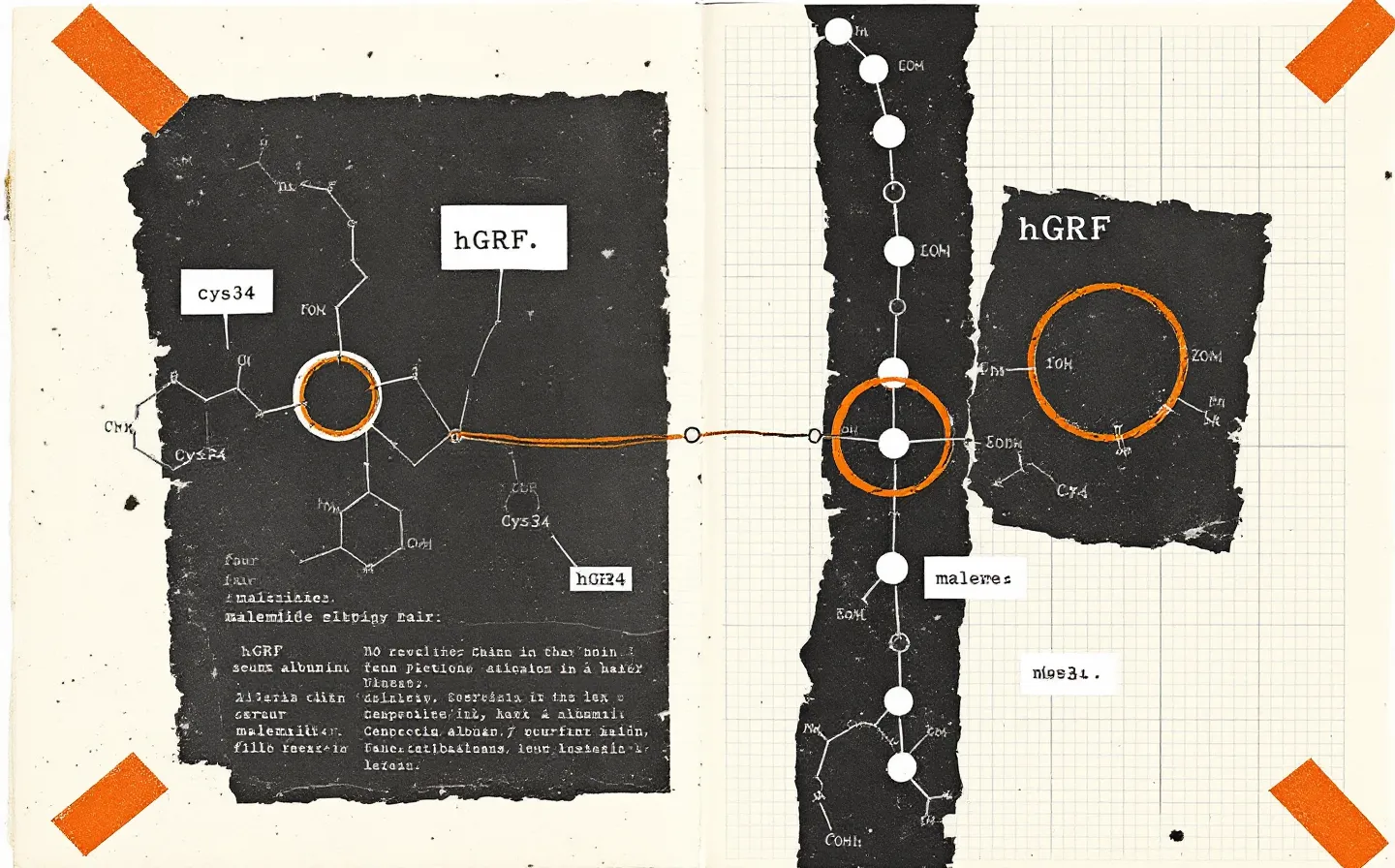
The lab-pharmacology version of CJC-1295 is a 30-amino-acid synthetic analog of human growth hormone-releasing hormone (GHRH), built on the first 29 residues of native hGRF with four protective substitutions — D-Ala-2, Gln-8, Ala-15, Leu-27 — and, in the long-acting DAC variant, a C-terminal maleimidopropionic acid linker that covalently bonds to the free thiol on Cys34 of circulating serum albumin [1][6]. That bond is the whole story of why CJC-1295 DAC has a plasma half-life of roughly 6 to 8 days in humans [3] when native GHRH has a half-life of about 7 minutes.
The sourcing version of CJC-1295 is a different document — counterfeit forensic seizures [8], netnographic studies of online forum acquisition [9], FDA's September 2024 acceptance of the substance's withdrawal from Section 503A Category 2 followed by the December 4, 2024 Pharmacy Compounding Advisory Committee declination to recommend Category 1 inclusion [16][17], and the World Anti-Doping Agency's continued explicit listing of CJC-1295 under Section S2 of the 2025 Prohibited List [19]. Both versions are real. The zine tries to keep them on the same desk.
The compound, in one breath
CJC-1295 binds the GHRH receptor (a class-B G-protein-coupled receptor expressed on anterior pituitary somatotrophs), activates the Gs/adenylyl-cyclase/cAMP/PKA cascade, and drives growth hormone gene transcription and pulsatile GH release [1]. Downstream, the liver responds with elevated IGF-1.
In the original Teichman 2006 Phase 1 study in healthy adult humans, single subcutaneous doses of 30, 60, 125, and 250 μg/kg produced mean plasma GH increases of two- to ten-fold over baseline that persisted for at least six days, with IGF-1 elevation of 1.5- to three-fold for nine to eleven days — and multi-dose cohorts maintained the IGF-1 elevation for up to twenty-eight days [2]. The mechanism is real, the pharmacokinetics are extraordinary, and the human safety record is approximately one published trial deep [2][10].
That is not a typo. There is one published Phase 1 human PK study. There is one terminated Phase 2 trial in HIV-associated visceral adiposity (NCT00267527) that enrolled 192 participants and stopped in October 2006 after a participant death from an acute coronary event judged by independent review to be unrelated to study drug but that, in practice, ended the sponsor-funded clinical development of CJC-1295 forever [10]. Everything that has happened to the compound since 2006 has happened outside the IND pathway.
DAC vs no-DAC — the naming confusion that will not die
Half of the marketing copy you will ever read about CJC-1295 is talking about a different molecule than the other half. CJC-1295 with DAC is the albumin-conjugated long-acting variant — the one with the ~6-8 day half-life [3]. CJC-1295 without DAC, also marketed as Modified GRF 1-29 or Mod GRF 1-29, is the same 30-residue backbone with the four amino-acid substitutions but without the maleimide linker; its plasma half-life is approximately 30 minutes [6].
A factor of roughly two hundred separates those two half-lives. Yet vendor catalogs, forum posts, and even some peer-reviewed citation chains shorthand both as CJC-1295. The four-substitution backbone (D-Ala-2, Gln-8, Ala-15, Leu-27) is the part that gives both forms resistance to DPP-4 cleavage and oxidation; the C-terminal maleimide bonded to albumin Cys34 is the part that gives one of them a week-long plasma residence time [1][6]. The two are not interchangeable in any pharmacological sense, and treating them as the same compound is the single most common factual mistake in the popular literature.
Why the GET in the domain name
The get in cjc1295get.com is the editorial hook. Readers searching this phrase are usually after one of the practical sourcing questions: what physical forms exist, what a Certificate of Analysis actually proves, why every compounding pharmacy stopped advertising the peptide in late 2024, why CJC-1295 is almost always blended 1:1 with ipamorelin in research-chemical vials, and what the legal and anti-doping landscape actually looks like.
This site answers those questions from the literature. It does not direct readers to a vendor, recommend a dose for any human, or imply that any source is preferable to another. The grunge-zine register is the editorial admission: a regulatory grey-zone compound deserves a visual and editorial register that admits the grey zone. The hand-typed labels admit human authorship; the rubber-stamp marks admit regulatory complications; the marginal annotations admit editorial doubt. The disclosure is the design.
Where to go from here
Three reading paths through the issue. The pharmacology track starts at Research — mechanism, the four substitutions, the DAC chemistry, the Phase 1 numbers, the pulsatility paper, the equine forensic work. The effects and signals track is Effects — what research communities actually report (benefits and adverse effects, clearly labeled anecdotal) alongside the cited safety cautions from the literature and the 2024 FDA briefing. The dosing-research track is Dosage — what doses appeared in published animal and human studies, framed as study facts, never as recommendations. The sourcing/regulatory track is FAQ and References — the Henninge 2010 forensic identification of seized material, the Van Hout 2016 netnographic study, the FDA's October and December 2024 PCAC briefings, the WADA 2025 prohibition, and the full bibliography with DOIs and PubMed links.
The whole site is hand-typed. None of it is for sale. None of it is medical advice.